
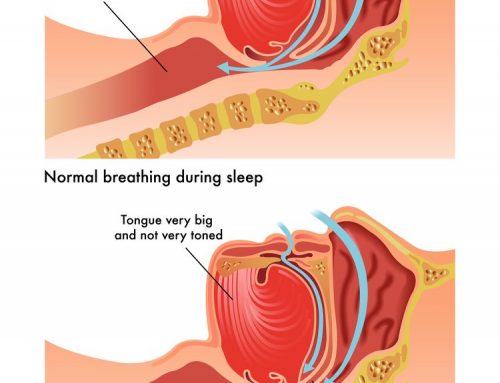
OSA affects 3-4% of the adult population and as much as 5-10% of the pediatric population. In OSA, there is usually snoring and also tissue collapse causing airway obstruction. This obstruction leads to decreased oxygen levels and frequent awakenings at night. Some people will have episodes of obstruction leading to arousal hundreds of times per night. As a result, sleep quality for OSA patients is quite poor and they are frequently very fatigued. Other common symptoms include concentration difficulty, memory impairment, and morning headaches. Children can potentially suffer decreased intelligence, hyperactivity disorders, bedwetting, and growth impairment. Importantly, OSA is linked to diabetes, coronary artery disease, hypertension, depression, and stroke.
Traditional Sleep Apnea Treatment
If sleep apnea is diagnosed, treatment must be initiated. In adults, first-line therapy is a continuous positive airway pressure (CPAP) device. CPAP works by forcing pressurized air into the patient’s nose and/or mouth, overpowering the obstruction in the throat and stenting it open. Many people have difficulty tolerating these devices. Other treatments include mandibular splints or surgery. If surgery is the chosen option, it is critical to identify the areas of obstruction in the nose and throat causing OSA. Some patients need nasal surgery (e.g., septoplasty, turbinate reduction, polyp removal). Others need their tonsils removed and soft palate trimmed. Other traditional surgeries include breaking the upper and lower jaws and advancing them forward.
Transoral Robotic Sleep Apnea Surgery
We have come to understand that sleep apnea is a multilevel obstruction in adult patients. The above named surgeries have not adequately addressed obstruction at the level of the tongue base or epiglottis. Older open surgeries for addressing these areas are morbid and require external incisions and longer hospital stays. Transoral robotic surgery (TORS) has revolutionized sleep apnea surgery by providing excellent visualization and access to lower areas of obstruction. We are now able to remove obstructive tongue base tissue in a precise manner that allows for no external incisions and short hospital stays. Full recovery takes approximately 3-4 weeks.
The system used is called the da Vinci®. It translates the surgeon’s movements to multiple robotic arms which carry out the actual surgery. The robotic instrumentation flexes at an artificial wrist allowing more movement and precise manipulation of tissue in tight areas. The robot also allows for increased vision for the surgeon due to innovative high definition camera placement and 3-D image modeling.
In order to be assessed for TORS sleep apnea surgery, patients are assessed in the office. Sleep study results are reviewed and the patient undergoes flexible laryngoscopic examination to identify the exact areas of obstruction. When the tongue base or epiglottis is identified as a site of obstruction, the patient is a candidate for the TORS sleep apnea procedure.
We are proud to announce that Dr. Robert Nason is one of only a handful of surgeons in the country performing TORS sleep apnea surgery. If you have sleep apnea, please schedule an appointment with ENT Specialists of Austin for a comprehensive evaluation to see if you are a candidate for robotic surgery.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Leave A Comment